Dr Leigh Martens
General Practitioner
Conditions Explained
Disclaimer:
This website is intended to assist with patient education and should not be used as a diagnostic, treatment or prescription service, forum or platform. Always consult your own healthcare practitioner for a more personalised and detailed opinion
Adult Forearm Fractures
We have selected the following expert medical opinion based on its clarity, reliability and accuracy. Credits: Sourced from the website OrthoInfo. Please refer to your own medical practitioner for a final perspective, assessment or evaluation.
What are adult forearm fractures?
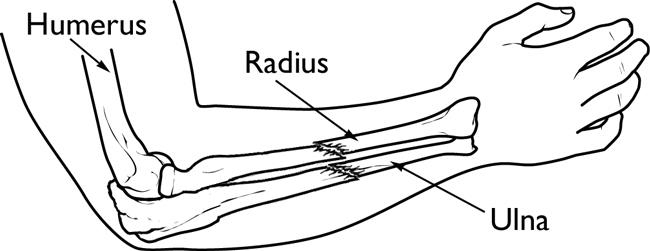
Your forearm is made up of two bones, the radius and ulna. In most cases of adult forearm fractures, both bones are broken.
Fractures of the forearm can occur near the wrist at the farthest (distal) end of the bone, in the middle of the forearm, or near the elbow at the top (proximal) end of the bone. This article focuses on fractures that occur in the middle segments of the radius and ulna. Fractures that involve the wrist or the elbow are discussed in separate articles.
Anatomy
If you hold your arms at your side with your palms facing up, the ulna is the bone closest to your body and the radius is closest to your thumb. The ulna is larger at the elbow — it forms the "point" of your elbow — and the radius is larger at the wrist.
The primary motion of the forearm is rotation: the ability to turn our palms up or down. The ulna stays still while the radius rotates around it. This is the motion used to turn a screwdriver or twist in a light bulb. Forearm fractures can affect your ability to rotate your arm, as well as bend and straighten the wrist and elbow.
Description
Forearm bones can break in several ways. The bone can crack just slightly, or can break into many pieces. The broken pieces of bone may line up straight or may be far out of place.
In some cases, the bone will break in such a way that bone fragments stick out through the skin or a wound penetrates down to the broken bone. This is called an open fracture and requires immediate medical attention because of the risk for infection.
Because of the strong force required to break the radius or ulna in the middle of the bone, it is more common for adults to break both bones during a forearm injury. When only one bone in the forearm is broken, it is typically the ulna — usually as a result of a direct blow to the outside of your arm when you have it raised in self defense.
Fractures of both the radius and ulna:
Cause
The most common causes of forearm fractures include:
- Direct blow
- Fall on an outstretched arm, often during sports or from a height
- Automobile/motorcycle accidents
Symptoms
A broken forearm usually causes immediate pain. Because both bones are usually involved, forearm fractures often cause an obvious deformity — your forearm may appear bent and shorter than your other arm. You will most likely need to support your injured arm with your other hand.
Additional symptoms include:
- Swelling
- Bruising (not as common as in other broken bones)
- Inability to rotate arm
- Numbness or weakness in the fingers or wrist (rare)
Doctor Examination
Most people with forearm fractures will go to an urgent care center or emergency room for initial treatment.
Physical Examination and Medical History
It is important that your doctor knows the circumstances of your injury. For example, if you fell from a ladder, how far did you fall? It is just as important for your doctor to know if you sustained any other injuries and if you have any other medical problems, such as diabetes. Your doctor also needs to know if you take any medications.
After discussing your symptoms and medical history, your doctor will do a careful examination. Your doctor will:
- Examine your skin to see if there are any cuts from the injury. Bone fragments can break through the skin and create lacerations. This leads to an increased risk for infection.
- Palpate (feel) all around your arm to determine if there are any other areas of tenderness. This can indicate other broken bones or injuries.
- Check your pulse at the wrist to be sure that good blood flow is getting through your forearm to your hand.
- Check to see if you can move your fingers and wrist, and can feel things with your fingers. Sometimes, nerves may be injured at the same time that the bone is broken, which can result in hand and wrist weakness and numbness.
- The doctor may examine your shoulder, upper arm, elbow, wrist, and hand, even if you only complain of arm pain.
X-rays
X-rays are the most common and widely available diagnostic imaging technique. X-rays can show if the bone is broken and whether there is displacement (the gap between broken bones). They can also show how many pieces of broken bone there are.
Treatment
Treatment of broken bones follows one basic rule: the broken pieces must be put back into position and prevented from moving out of place until they are healed. Because the radius and ulna rely on each other for support, it is important that they are properly stabilized. If the bones are not accurately aligned during healing, it may result in future problems with wrist and elbow movement.
Most cases of adult forearm fractures require surgery to make sure the bones are stabilized and lined up for successful healing.
Immediate Treatment
While you are in the emergency room, the doctor may try to temporarily realign the bones, depending upon how far out of place the pieces are. "Reduction" is the technical term for this process in which the doctor moves the pieces into place. This is not a surgical procedure. Your pain will be controlled with medication. Afterward, your doctor will apply a splint (like a cast) to your forearm and provide a sling to keep your arm in position. Unlike a full cast, a splint can be tightened or loosened, and allows swelling to occur safely.
The emergency room doctor may apply a splint to protect your arm:

Reproduced with permission from JF Sarwark, ed: Essentials of Musculoskeletal Care, ed 4. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2010.
It is very important to control the movement of a broken bone. Moving a broken bone can cause additional damage to the bone, nearby blood vessels, and nerves or other tissues surrounding the bone.
Additional immediate treatment will include applying ice to help reduce swelling, and providing you with pain medicine.
Nonsurgical Treatment
If only one bone is broken and it is not out of place, it may be possible to treat it with a cast or brace. Your doctor will closely monitor the healing of the fracture, and have you return to the clinic for x-rays frequently. If the fracture shifts in position, you may require surgery to put the bones back together.
Surgical Treatment
When both forearm bones are broken, or if the bones have punctured the skin (open fracture), surgery is usually required.
Because of the increased risk for infection, open fractures are usually scheduled for surgery immediately. Patients are typically given antibiotics by vein (intravenous) in the emergency room, and may receive a tetanus shot. During surgery, the cuts from the injury will be thoroughly cleaned out. The broken bones are typically fixed during the same surgery.
If the skin around your fracture has not been broken, your doctor may recommend waiting until swelling has gone down before having surgery. Keeping your arm immobilized and elevated for several days will decrease swelling. It also gives skin that has been stretched a chance to recover.
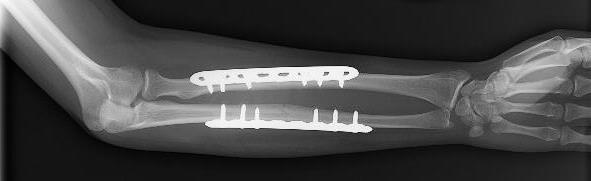
Open reduction and internal fixation with plates and screws: This is the most common type of surgical repair for forearm fractures. During this type of procedure, the bone fragments are first repositioned (reduced) into their normal alignment. They are held together with special screws and metal plates attached to the outer surface of the bone.
Open reduction and internal fixation with rods: During this procedure, a specially designed metal rod is inserted through the marrow space in the center of the bone.
External fixation: If the skin and bone are severely damaged, using plates and screws and large incisions may injure the skin further. This may result in infection. In this case, you may be treated with an external fixator. In this type of operation, metal pins or screws are placed into the bone above and below the fracture site. The pins and screws are attached to a bar outside the skin. This device is a stabilizing frame that holds the bones in the proper position so they can heal.
The broken bones of the forearm are held in position by plates and screws while they heal:
Complications
Complications from Forearm Fractures
Forearm fractures can cause further injury and complications:
- The ends of broken bones are often sharp and can cut or tear surrounding blood vessels or nerves.
- Excessive bleeding and swelling right after the injury may lead to acute compartment syndrome, a condition in which the swelling cuts off blood supply to the hand and forearm. It typically occurs within 24 to 48 hours of the injury and causes severe pain when moving the fingers. Compartment syndrome can result in loss of sensation and function, and requires emergency surgery once it is diagnosed. In such cases, the skin and muscle coverings are opened and left open to relieve pressure and allow blood to return.
- Open fractures expose the bone to the outside environment. Even with good surgical cleaning of the bone and muscle, the bone can become infected. Bone infection is difficult to treat and often requires multiple surgeries and long-term antibiotics.
Complications from Surgery
There are risks associated with all surgery. If your doctor recommends surgery, he or she thinks that the possible benefits of surgery outweigh the risks.
- Infection: There is a risk of infection with any surgery, whether it is for a forearm fracture or another purpose.
- Damage to nerves and blood vessels: There is a minor risk of injury to nerves and blood vessels around the forearm. Although some temporary numbness is common right after your injury, if you experience persistent numbness or tingling in your fingers, contact your doctor.
- Synostosis: Another rare complication is healing between the two bones of the forearm with a bridge of bone known as synostosis. This can decrease the rotation of the bones and prevent full movement.
- Nonunion: Surgery does not guarantee healing of the fracture. A fracture may pull apart, or the screws, plates, or rods may shift or break.
This can occur for a variety of reasons, including:- The patient does not follow directions after surgery.
- The patient has other health issues that slow healing. Some diseases, like diabetes, slow healing. Smoking or using other tobacco products also slow healing.
- If the fracture was associated with a cut in the skin (an open fracture), healing is often slower.
- Infections can also slow or prevent healing.
If the fracture fails to heal, further surgery may be needed.
Recovery
Bones have a remarkable capacity to heal. Forearm bones typically take 3 to 6 months to fully heal. The more severe your injury, however, the longer your recovery may be.
Pain Management
Pain after an injury or surgery is a natural part of the healing process. Your doctor and nurses will work to reduce your pain, which can help you recover faster.
Medications are often prescribed for short-term pain relief after surgery or an injury. Many types of medicines are available to help manage pain, including opioids, non-steroidal anti-inflammatory drugs (NSAIDs), and local anesthetics. Your doctor may use a combination of these medications to improve pain relief, as well as minimize the need for opioids.
Be aware that although opioids help relieve pain after surgery or an injury, they are a narcotic and can be addictive. It is important to use opioids only as directed by your doctor. As soon as your pain begins to improve, stop taking opioids. Talk to your doctor if your pain has not begun to improve within a few days of your treatment.
Rehabilitation
Nonsurgical treatment: Rehabilitation typically begins after a few weeks of keeping the arm still by using a cast or brace. In many cases, a physical therapist will help with rehabilitation, beginning with gentle exercises to increase range of motion, and gradually adding exercises to strengthen the arm.
Surgical treatment: Depending on the complexity of the fracture and the stability of the repair, a cast or brace may be necessary for 2 to 6 weeks after surgery. Motion exercises for the forearm, elbow, and wrist usually begin shortly after surgery. This early motion is important to prevent stiffness. Your doctor may also prescribe visits to a physical or occupational therapist, depending on how long your arm was immobilized.
Outcome
Some stiffness after healing is common, but this does not usually affect the overall function of your arm.
Your doctor will advise you on when you may return to work and sports activities. This varies depending on the fracture pattern and the type and stability of the repair.
If you have had surgery, the plates and screws are usually left in place forever. If you consider removal, this second surgery is typically not scheduled until your bones have fully solidified (1 to 2 years after initial surgery).
_______________________________________________________________________________________________________________________
Are you a healthcare practitioner who enjoys patient education, interaction and communication?
If so, we invite you to criticise, contribute to or help improve our content. We find that many practicing doctors who regularly communicate with patients develop novel and often highly effective ways to convey complex medical information in a simplified, accurate and compassionate manner.
MedSquirrel is a shared knowledge, collective intelligence digital platform developed to share medical expertise between doctors and patients. We support collaboration, as opposed to competition, between all members of the healthcare profession and are striving towards the provision of peer reviewed, accurate and simplified medical information to patients. Please share your unique communication style, experience and insights with a wider audience of patients, as well as your colleagues, by contributing to our digital platform.
Your contribution will be credited to you and your name, practice and field of interest will be made visible to the world. (Contact us via the orange feed-back button on the right).