Back Conditions Explained
Enlarged Prostate – BPH
Also known as "Prostate Gland Enlargement" or "Benign Prostatic Hyperplasia (BPH)"
We have selected the following expert medical opinion based on its clarity, reliability and accuracy. Credits: Sourced from the website Patient UK, authored by Dr Laurence Knott (see below). Please refer to your own medical practitioner for a final perspective, assessment or evaluation.
Overview
The prostate gland commonly becomes larger in older men. This prostate gland enlargement is also called benign prostatic hyperplasia (BPH). It can cause problems with passing urine. Symptoms are often mild. Without treatment, symptoms do not always become worse and may even improve over time. If symptoms become troublesome or distressing they can be improved by medicines or surgery.
What is the prostate gland?
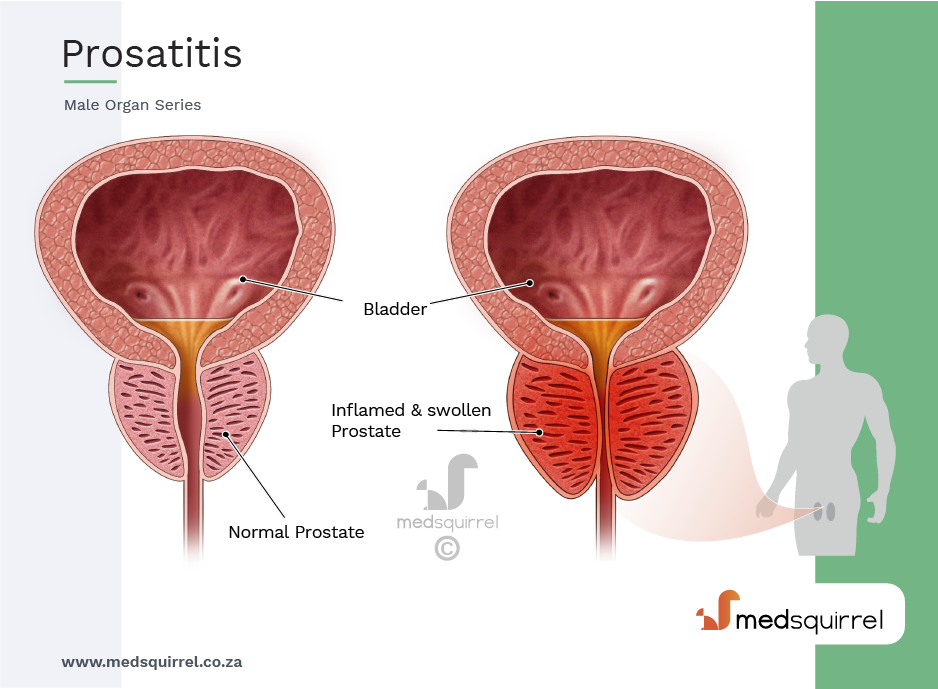
The prostate gland (just called prostate from now on) is only found in men. It lies just beneath the bladder. It is normally about the size of a chestnut. The tube which passes urine from the bladder (the urethra) runs through the middle of the prostate. The prostate's main function is to produce fluid which protects and enriches sperm.
The prostate gets bigger (enlarges) gradually after the age of about 50. By the age of 90, about 9 in 10 men have an enlarged prostate.
Symptoms
What are the symptoms of prostate enlargement?
The symptoms of prostate enlargement are called lower urinary tract symptoms (LUTS). LUTS can also be caused by other conditions.
As the prostate enlarges it may cause narrowing of the urethra. This may partially obstruct the flow of urine.
This can lead to obstructive symptoms such as:
- Poor stream: The flow of urine is weaker, and it takes longer to empty your bladder.
- Hesitancy: You may have to wait at the toilet for a while before urine starts to flow.
- Dribbling: Towards the end of passing urine, the flow becomes a slow dribble.
- Poor emptying: You may have a feeling of not quite emptying your bladder.
The enlarged prostate may also make the bladder irritable, which may cause:
- Frequency: You may pass urine more often than normal. This can be most irritating if it happens at night. Getting up several times a night to pass urine is a common symptom and is called nocturia.
- Urgency: This means you have to get to the toilet quickly when you need to go.
Usually the symptoms are mild to begin with - perhaps a slightly reduced urine flow or having to wait a few seconds to start passing urine. Over months or years, the symptoms may become more troublesome and severe. Complications develop in some cases.
Note 1: an enlarged prostate does not always cause symptoms. Only a quarter to a half of men with an enlarged prostate will have symptoms. Also, the severity of the symptoms is not always related to the size of the prostate. It depends on how much the prostate obstructs the urethra.
Note 2: not all urinary symptoms in men are due to an enlarged prostate. In particular, if you pass blood, become incontinent, or have pain, it may be due to bladder, kidney or other prostate conditions. You should see a doctor if these symptoms occur.
Complications
What are the possible complications?
Urinary symptoms do not worsen in everyone. Serious complications are unlikely to occur in most men with an enlarged prostate.
Complications that sometimes occur include:
- In some cases, a total blockage of urine occurs so you will no longer be able to pass urine. This is called urinary retention. It can be very uncomfortable, and you will need to have a small tube (catheter) inserted to drain the bladder. It occurs in less than 1 in 100 men with an enlarged prostate each year.
- In some cases, only some of the urine in the bladder is emptied when you pass urine. Some urine remains in the bladder at all times. This ongoing condition is called chronic retention. This may cause repeated (recurring) urine infections, or incontinence (as urine dribbles around the blockage rather than large amounts being passed each time you go to the toilet).
Note: the risk of prostate cancer is not increased. Men with a benign prostate enlargement are no more or less likely to develop prostate cancer than those without benign prostate enlargement.
Diagnosis
Do I need any tests?
Benign prostatic enlargement is usually diagnosed based on the typical symptoms as described earlier. Tests are not needed to confirm the diagnosis but to make sure no complications have developed. Tests are also useful in ruling out other causes of your symptoms and sometimes give the doctor an idea of the size of your prostate.
The following tests may be done:
- A doctor may examine your prostate to see how big it is. This is done by inserting a gloved finger into your back passage (through the anus into the rectum) to feel the back of the prostate gland. The size of your bladder may be assessed by examining your tummy (abdomen).
- Urine and blood tests may be done to check the function of your kidneys, to exclude a urine infection and to check there is no blood in the urine.
- A referral to a bladder specialist (urologist) may be advised if your symptoms are troublesome or if complications develop.
Tests may be done in these more severe cases, particularly if surgery is being considered as a treatment. For example:
- A look inside the bladder with a special telescope (cystoscopy).
- A urine flow test to assess how bad the obstruction has become.
- An ultrasound scan to see whether much urine remains in the bladder after you pass urine (void).
- Voiding diary: You may be asked to complete a diary over a week or so. This will have information about the number of times during the day and night you void, the amount passed and also the number and types of drinks you have had.
- A prostate specific antigen (PSA) blood test may be offered, although this test is not done routinely. This can be used as a marker for the size of the prostate. Larger prostates make more PSA.
Note: a high PSA level is also found in people with prostate cancer. It has to be stressed that most men with prostate symptoms do not have prostate cancer.
Treatment
Is treatment always necessary?
No. In most cases, an enlarged prostate does not do any damage or cause complications. Whether treatment is needed usually depends on how much bother the symptoms cause. For example, you may be glad for some treatment if you are woken six times a night, every night, with an urgent need to go to the toilet. On the other hand, slight hesitancy when you go to the toilet and getting up once a night to pass urine may cause little problem and not need treatment.
What are the treatment options for prostate enlargement?
Enlarged Prostate Management Options:
Each treatment option for an Enlarged Prostate has various benefits, risks and consequences. No treatment is likely to clear all symptoms totally, although symptoms can usually be greatly improved with treatment. The treatments considered usually depend on how severe and bothersome your symptoms are.
General measures
The following tips may help if you opt not to have treatment (for example, if symptoms are mild) or if treatment does not fully work:
- Try to anticipate times when urinary frequency and urgency are likely to be most inconvenient and reduce the amount that you drink beforehand. For example, when you go out, don't drink much for 2-3 hours before you go out. However, do not reduce the total amount of fluid to less than 1.5 litres each day.
- After you have finished passing urine, go back to the toilet again after a few minutes to try to pass some more. (This is called double micturition.) This aims to make sure the bladder is emptied completely.
- Consider reducing or stopping caffeine (commonly found in tea, coffee and cola) and alcohol. These can make the symptoms of frequency, urgency and getting up several times a night to pass urine (nocturia) worse.
- If hesitancy is a problem - try to relax when standing to pass urine.
- If urgency is a problem - try some distraction techniques such as breathing exercises and mental tricks (for example, counting) to take your mind off the bladder.
- If frequency is a problem - try retraining the bladder by holding on for as long as you can each time before passing urine. The bladder muscle can be trained to expand more in this way. Eventually, the bladder may be trained to hold on for longer each time before you need to go to the toilet.
- If you are a smoker then stopping smoking may significantly improve your symptoms, as nicotine irritates the bladder.
Not treating may be an option (often called watchful waiting)
If symptoms are mild, then this may be the best option. You may be happy just to see how things go if the symptoms are not too bothersome and are not affecting your life very much. The situation can be reviewed every year or so, or sooner if there is change in symptoms. Symptoms do not always become worse. They may even improve.
Medicines
The decision to treat with medicines usually depends on how much bother the symptoms are causing you. There are two groups of medicines that may help: alpha-blockers and 5-alpha reductase inhibitors. Medicines do not cure the problem, nor do they usually make symptoms go completely. However, symptoms often ease if you take a medicine.
Alpha-blocker medicines:
These medicines work by relaxing the smooth muscle of the prostate and bladder neck. This can improve the flow of urine. There are several different types and brands of alpha-blockers which include prazosin, indoramin, tamsulosin, alfuzosin, doxazosin and terazosin. There is no real difference between how effective these medicines are, but some tend to cause side-effects more often than others. In most cases, symptoms improve with taking an alpha-blocker. However, the amount of improvement varies from person to person. Some improvement usually occurs within a few days, but the full effect may take up to six weeks.
Although side-effects are uncommon, they occur in some people. The most common side-effects are slight drowsiness, headaches and dizziness. If you are prescribed an alpha-blocker, read the leaflet that comes with the medicine packet for a full list of possible side-effects and cautions.
5-alpha reductase inhibitor medicines:
These are alternatives to alpha-blockers. There are two: finasteride and dutasteride. These work by blocking the conversion of the hormone testosterone to dihydrotestosterone in the prostate.
They do this by blocking a chemical (an enzyme) called 5-alpha-reductase. Dihydrotestosterone is partly responsible for making the prostate enlarge. Therefore, a reduced amount of dihydrotestosterone in the prostate causes it to shrink. These medicines have been shown in studies to improve prostate symptoms, reduce the risk of complications and also reduce the need for surgery.
It can take up to six months for you to notice any effect from these medicines, as it takes time for the prostate gradually to shrink.
It is unusual to have side-effects with 5-alpha reductase inhibitor medicines. However, a small proportion of men may have impotence and reduced sex drive. With finasteride, these side-effects occur shortly after you start taking the tablets and disappear if you persevere with them. With dutasteride, these side-effects may continue even after treatment is stopped.
Which medicine is chosen?
The severity of symptoms is not always related to the size of the prostate. A small or large enlargement may cause mild or severe symptoms. An alpha-blocker may help, whatever the size of the prostate, as it works by relaxing muscle fibres. Finasteride or dutasteride tend to work best if you have a larger prostate which has more tissue to shrink. Your doctor will advise which medicine may be best in your circumstances. Also, if you develop a problem or side-effect with one type of medicine then another may be an option.
Combinations of medicines:
In some cases, a combination of an alpha-blocker plus a 5-alpha reductase inhibitor is used. This may give quicker and better relief of symptoms than either alone. Some studies suggest that in men who take a combination of two medicines, about four in five men can stop the alpha-blocker after 6-12 months without their symptoms getting any worse. This is likely to be because the prostate will have shrunk with the 5-alpha reductase inhibitor after this time and the alpha-blocker is no longer then needed.
Herbal remedies
There is currently no strong evidence that herbal remedies improve the symptoms due to an enlarged prostate. More studies are needed in this area.
Surgery
Removal of part of the prostate is an option if symptoms are very bothersome or if medicines do not help. Around one in four men with an enlarged prostate will have an operation at some stage. In these operations, only the central part of the prostate is removed (creating a wide channel for urine to flow through), leaving the outer part behind. This is different to prostate cancer when, if surgery is carried out for cure, all the prostate is removed.
There are many different types of operation now available that can remove prostate tissue. Your surgeon will discuss the most suitable operation for you in more detail. Some of the more commonly done operations are listed below:
Transurethral resection of the prostate (TURP):
This is the most common operation carried out for an enlarged prostate. Under anaesthetic, either spinal or general, a rigid cystoscope is inserted through the urethra into the bladder. A cystoscope is a narrow tube-like telescope through which small instruments pass to allow the operation to be carried out. A semi-circular loop of wire has an electrical current passed through it. It is this loop that sticks out from the end of the cystoscope and cuts out small chips of prostate that are then washed out at the end of the operation. This operation nearly always gives good relief of symptoms. 80-90% of men after this operation will have retrograde ejaculation. This means that semen goes backwards into the bladder at climax producing a 'dry' orgasm. Impotence and incontinence are rare complications after a TURP.
Transurethral incision of the prostate (TUIP):
This may be offered if you only have a slightly enlarged prostate. For this operation, the surgeon makes small cuts in the prostate where the prostate meets the bladder. This then relaxes the opening to the bladder, resulting in there being an improved flow of urine out of the bladder. There is less risk of retrograde ejaculation with this operation.
Open prostatectomy:
This is a more traditional operation which involves cutting the skin to get to the prostate. It is now rarely done. It is only performed when the prostate is very large and when it would not be practicable to remove an adequate amount of prostate tissue through a narrow cystoscope inserted through the urethra.
Laser prostatectomy:
This is simply the application of newer technologies to achieve the same goal as either TURP or open prostatectomy. It has the advantage of fewer side-effects, a shorter period of having a catheter in and a shorter stay in hospital (often just one night).
There are two types of lasers:
- Green light which vaporises the prostate tissue to create a cavity
- Holmium or thulium lasers that can very effectively core out large pieces (lobes) of prostate which, in turn, are chopped into small pieces in order to be removed from the bladder.
In the hands of experienced laser surgeons, very large prostates, which in the past could only be dealt with by open surgery, can be removed by this technique.
Other methods:
Implants can be used to lift the urethra and improve flow of urine. This procedure has been shown to have fewer problems with sexual function than TURP. Other forms of energy are also being investigated instead of lasers. These include microwaves, radiofrequency waves, high-intensity ultrasound and high-voltage electrical energy. Research continues to find new ways to manage these symptoms and you may be offered a chance to take part in these studies.
About the author
Dr Laurence Knott
BSc (Hons) (Biochemistry), MB BS
Qualified 1973. 37 years experience in general practice. Medical author who has contributed to many lay and professional publications. Particularly interested in converting medical terminology into information comprehensive to non-medical readers. Clinical complaints adviser to the Medical Defence Union. External professional adviser to the Health Service Ombudsman. Extensive medicolegal practice specialising in clinical negligence. Listed on the National Crime Database, advising police forces and the Crown Prosecution Service on medicolegal aspects of criminal cases. Erstwhile GP medical adviser to the Guillain-Barré & Associated Inflammatory Neuropathies charity, now member and ex-patient.
Recommended websites
For further reading go to:
_______________________________________________________________________________________________________________________
Are you a healthcare practitioner who enjoys patient education, interaction and communication?
If so, we invite you to criticise, contribute to or help improve our content. We find that many practicing doctors who regularly communicate with patients develop novel and often highly effective ways to convey complex medical information in a simplified, accurate and compassionate manner.
MedSquirrel is a shared knowledge, collective intelligence digital platform developed to share medical expertise between doctors and patients. We support collaboration, as opposed to competition, between all members of the healthcare profession and are striving towards the provision of peer reviewed, accurate and simplified medical information to patients. Please share your unique communication style, experience and insights with a wider audience of patients, as well as your colleagues, by contributing to our digital platform.
Your contribution will be credited to you and your name, practice and field of interest will be made visible to the world. (Contact us via the orange feed-back button on the right).
Disclaimer:
MedSquirrel is a shared knowledge, collective intelligence digital platform developed to share medical knowledge between doctors and patients. If you are a healthcare practitioner, we invite you to criticise, contribute or help improve our content. We support collaboration among all members of the healthcare profession since we strive for the provision of world-class, peer-reviewed, accurate and transparent medical information.
MedSquirrel should not be used for diagnosis, treatment or prescription. Always refer any questions about diagnosis, treatment or prescription to your Doctor.